CRYOLIPOLYSIS FOR SUBCUTANEOUS FAT LAYER REDUCTION | Ingargiola
Michael J. Ingargiola, M.D., Saba Motakef, M.D., Michael T. Chung, M.D., Henry C. Vasconez, M.D., and Gordon H. Sasaki, M.D.
Plast Reconstr Surg. 2015 Jun; 135(6): 1581–1590.
Contents
Abstract
Background:
Cryolipolysis is a nonsurgical technique for localized fat reduction. With the increased risk of complications from more invasive methods such as liposuction, cryolipolysis presents a promising method for nonsurgical body contouring. This study presents a systematic review of the available clinical data, with an emphasis on the efficacy, methods, safety, and complications of cryolipolysis.
Methods:
To identify clinical studies that assessed outcomes of cryolipolysis, a systematic review of the MEDLINE and Cochrane databases was performed with the search algorithm cryolipolysis OR cool sculpting OR fat freezing OR lipocryolysis.
Results:
The primary literature search returned 319 articles. After inclusion criteria were applied and additional articles were idenfied via manual review of article references, 19 studies were selected for review. Average reduction in caliper measurement ranged from 14.67 percent to 28.5 percent. Average reduction by ultrasound ranged from 10.3 percent to 25.5 percent. No significant impact on lipid levels or liver function tests after cryolipolysis treatments was noted in any study. Only mild, short-term side effects, such as erythema, swelling, and pain, were noted. Paradoxical adipose hyperplasia was described in one patient.
Conclusions:
Cryolipolysis is a promising procedure for nonsurgical fat reduction and body contouring and presents a compelling alternative to liposuction and other, more invasive methods. This procedure appears to be safe in the short term, with a limited side effect profile, and results in significant fat reduction when used for localized adiposities. It remains unclear whether posttreatment manual massage and multiple treatments in the same anatomic area enhance the efficacy of cryolipolysis.
INTRODUCTION
Body contouring remains among the most common cosmetic surgical procedures performed in the United States. Data from the American Society for Aesthetic Plastic Surgery indicate that liposuction replaced breast augmentation as the most popular surgical procedure in 2013, with 363,912 procedures performed. Its popularity has grown considerably because of advantages such as aesthetic improvements as well as numerous metabolic benefits.1,2 Despite its popularity, there remain rare but significant risks regarding liposuction, including complications from anesthesia, infections, and even death.3 Clinical studies have reported a 21.7 percent incidence of minor complications as well as a 0.38 percent incidence of major complications.4,5 Similarly, Fischer et al. showed that the incidence of minor wound complications was 6.3 percent, and the incidence of a major morbidity was 6.8 percent within 30 days after a surgical body contouring procedure.6
Although liposuction is an effective therapeutic option for the removal of excess adipose tissue, it remains an invasive procedure and carries the inherent risks associated with surgery. In recent years, new modalities have been developed to address body contouring from a less-invasive perspective. These modalities primarily target the physical properties of fat that differentiate it from the overlying epidermis and dermis, thus resulting in selective destruction of fat. Devices using high-frequency ultrasound, radiofrequency energy, and laser light have the potential to improve efficiency, minimize adverse consequences, and shorten postoperative recovery time. Through thermal destruction, cavitational destruction, or creation of a temporary adipocyte cell membrane pore, the final result is that the number of adipocytes is reduced, which, when translated over millions of fat cells, results in a measurable reduction of fat.7
Cryolipolysis is one of the most recent forms of noninvasive fat reduction to emerge. The development behind cryolipolysis stems from the clinical observation of cold-induced panniculitis.8–10 In 1970, Epstein and Oren coined the term popsicle panniculitis after reporting the presence of a red indurated nodule followed by transient fat necrosis in the cheek of an infant who had been sucking on a popsicle.9 Initially described in infants, cold-induced panniculitis has also been observed in adult patients. These observations led to the concept that lipid-rich tissues are more susceptible to cold injury than the surrounding water-rich tissue. With these historical observations in mind, Manstein et al. introduced a novel noninvasive method for fat reduction with freezing in 2007, termed cryolipolysis.11 This technique is performed by applying an applicator to the targeted area set at a specific cooling temperature for a preset period of time. This targets adipocytes while sparing the skin, nerves, vessels, and muscles.
Initial preclinical and clinical studies have demonstrated the efficacy of cryolipolysis for subcutaneous fat layer reduction. However, the exact mechanism of action for cryolipolysis is not yet completely understood. In addition, the techniques of cryolipolysis treatment are not uniformly applied. Studies have suggested that the addition of posttreatment manual massage may enhance the effectiveness of a single cryolipolysis treatment, and that multiple treatments may lead to further improvement.12,13 Finally, we are currently still unaware of the long-term side effects and outcomes of this treatment. The aim of the present review was to give an overview of cryolipolysis with emphasis on the efficacy (volume reduction), methods, safety, and complications.
PATIENTS AND METHODS
Search Strategy, Article Selection, and Data Extraction
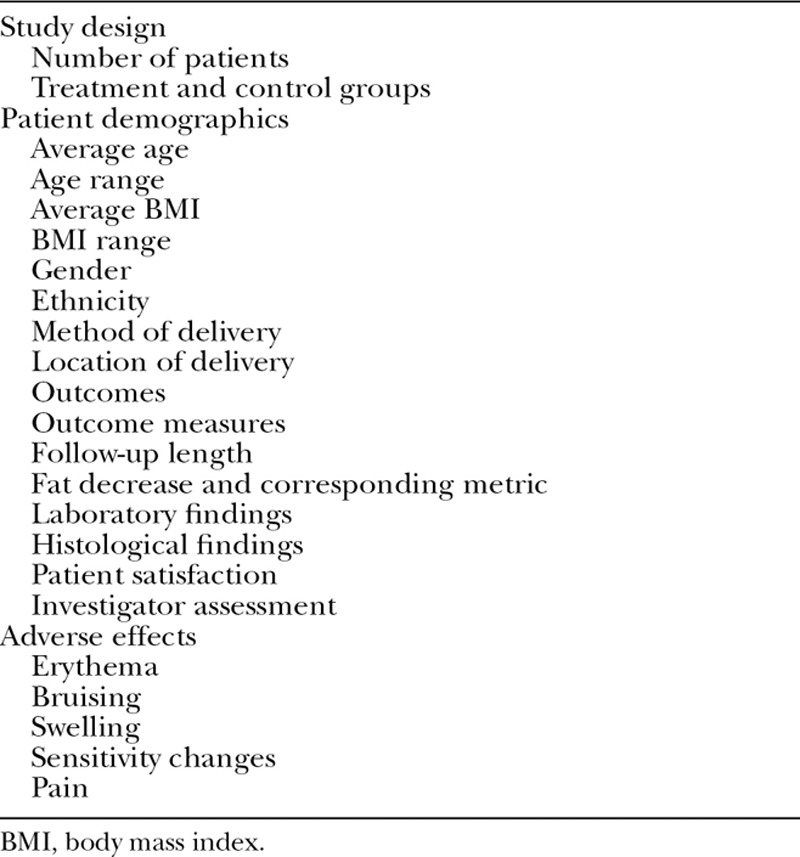
A systematic review of the MEDLINE and Cochrane databases was performed with the search algorithm cryolipolysis OR cool sculpting OR fat freezing OR lipocryolysis. Two investigators independently reviewed article titles and abstracts to identify studies that assessed outcomes of cryolipolysis. Selected articles that met these inclusion criteria then underwent full article review by the two investigators. Additional articles were then identified by manual review of the references of the articles that were initially identified via the primary search. Review papers and animal studies were eliminated. A third investigator reconciled disagreements. The Cohen Kappa coefficient was calculated to demonstrate the level of agreement between the two initial investigators. The same two investigators performed data extraction independently, and any discrepancies were again reconciled by the third. Table 1 lists the information extracted from each article.
RESULTS
Search Strategy and Article Selection
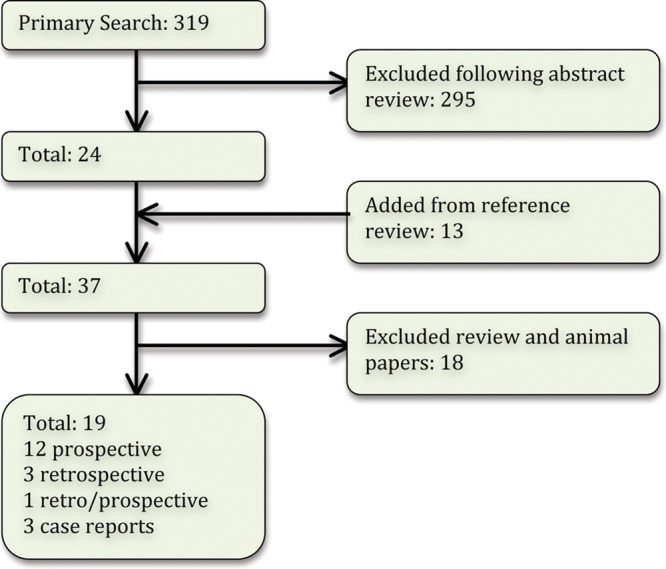
The primary literature search returned 319 articles (Fig. 1). The references of articles identified in the primary search were reviewed, yielding a total of 37 articles. Review papers and animal studies were eliminated, yielding a final number of 19 articles, including 12 prospective studies, three retrospective studies, one study with both prospective and retrospective groups, and three case reports. The Kappa coefficient was calculated at 0.885, indicating very good agreement between the investigators.
Efficacy
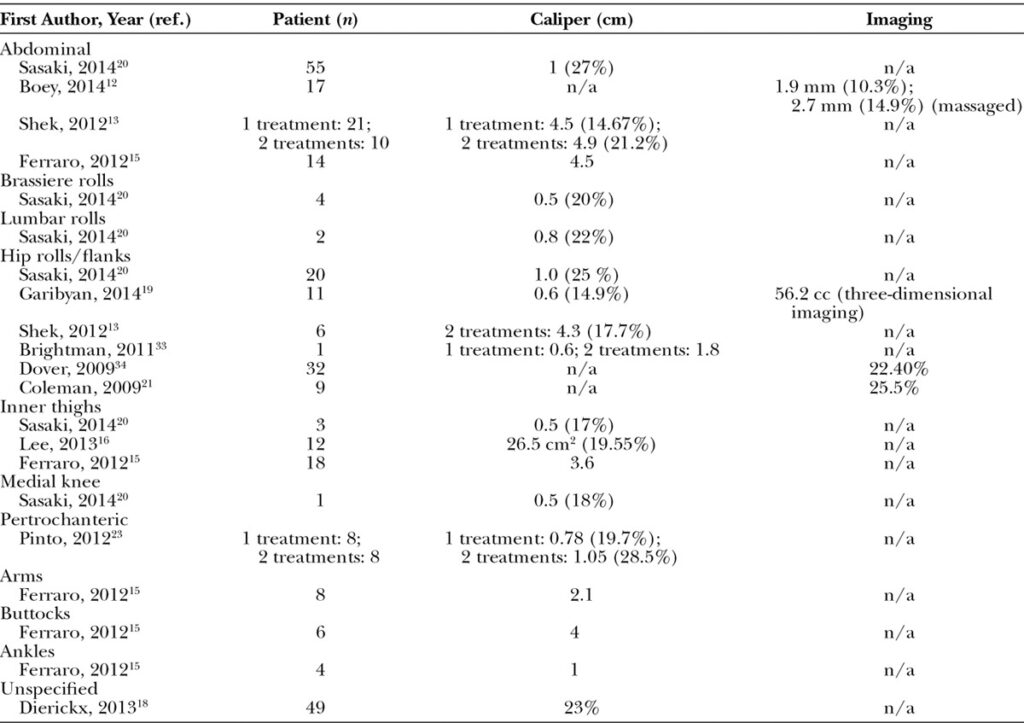
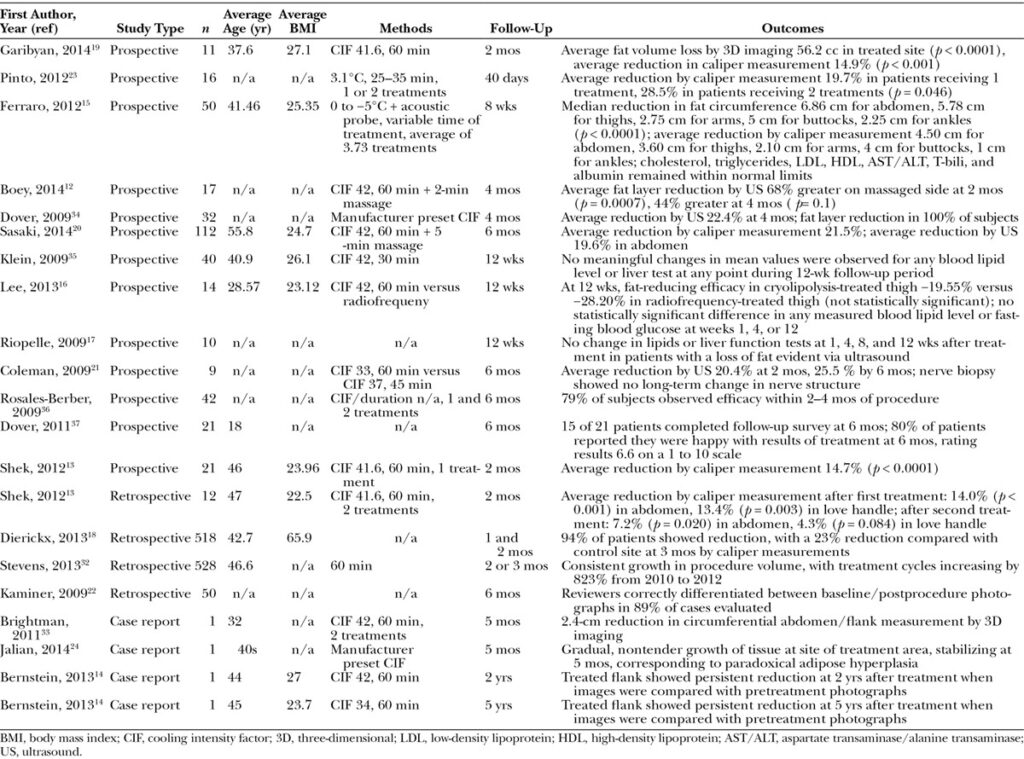
Common treatment areas included the abdomen, brassiere rolls, lumbar rolls, hip rolls/flanks, inner thighs, medial knee, peritrochanteric areas, arms, and ankles (Table .2). Follow-up length generally ranged from 2 to 6 months, although one study presented case reports on two patients at 2 and 5 years after treatment,14 noting persistent reduction at these time points when comparing pretreatment and post treatment photographs. Objective outcome measures included fat caliper measurements, ultrasound measurements, and three-dimensional imaging (VECTRA M3; Canfield Scientific, Inc., Fairfield, N.J.). Every study that evaluated clinical outcomes using these outcome measures noted a significant reduction in fat volume in treatment areas (Table .3). Although outcomes varied greatly based on treatment site and study design, average reduction in caliper measurement ranged from 14.67 percent to 28.5 percent. Average reduction by ultrasound ranged from 10.3 percent to 25.5 percent (Table .3). Three studies evaluated lipid levels and liver function tests (Table 33.15–17 No significant impact was noted on lipid levels or liver function tests after cryolipolysis treatments in any study.
DISCUSSION
Recently, a surge of novel technologies involving noninvasive, energy-based techniques have been introduced to the market, signaling a potential paradigm shift in fat reduction and body contouring practices. The major goal of these novel therapies includes volume reduction of tissue, with a possible end point of noninvasive body contouring.25 With more than 450,000 procedures performed thus far, cryolipolysis is becoming one of the most popular alternatives to liposuction for spot reduction of adipose tissue.26 Because of its ease of use and limited adverse effects, this procedure is becoming the leading technology in noninvasive techniques as well. This review sought to explore the efficacy, methods, safety, and complications of cryolipolysis in the current literature.
Although its mechanism is not fully understood, it is believed that vacuum suction with regulated heat extraction impedes blood flow and induces crystallization of the targeted adipose tissue when cryolipolysis is performed.11,27 The temperatures induced in cryolipolysis have no permanent effect on the overlying dermis and epidermis. However, this cold ischemic injury may promote cellular injury in adipose tissue via cellular edema, reduced Na-K-ATPase activity, reduced adenosine triphosphate, elevated lactic acid levels, and mitochondrial free radical release.20 Another mechanism proposes that the initial insult of crystallization and cold ischemic injury induced by cryolipolysis is further compounded by ischemia reperfusion injury, causing generation of reactive oxygen species, elevation of cytosolic calcium levels, and activation of apoptotic pathways.20 Ultimately, crystallization and cold ischemic injury of the targeted adipocytes induce apoptosis of these cells and a pronounced inflammatory response, resulting in their eventual removal from the treatment site within the following several weeks.7,11,25 Histological studies show that within 3 months, macrophages are mostly responsible for clearing the damaged cells and debris.26,28
With the removal of the adipocytes internally, there has been concern that cryolipolysis may cause rising blood lipid levels and elevations in liver enzymes that may put the patient at additional risk, particularly for cardiovascular parameters. However, multiple studies have demonstrated that cholesterol, triglycerides, low-density lipoprotein, high-density lipoprotein, aspartate transaminase/alanine transaminase, total bilirubin, albumin, and glucose remained within normal limits during and after cryolipolysis.15–17
With the relatively recent emergence of cryolipolysis, many factors still need to be considered and investigated, including what type of patient would benefit most from this procedure. Ferraro et al. suggested that patients who require only small or moderate amounts of adipose tissue and cellulite removal would benefit most from cryolipolysis treatment.15 Contraindications to cryolipolysis include cold-induced conditions such as cryoglobulinemia, cold urticaria, and paroxysmal cold hemoglobinuria.29 Cryolipolysis should not be performed in treatment areas with severe varicose veins, dermatitis, or other cutaneous lesions.23,27
Although all studies reviewed showed a fat reduction in every area examined, it is still unknown what areas are most responsive to cryolipolysis. Various factors may play a role in the degree of fat reduction observed after cryolipolysis. The vascularity, local cytoarchitecture, and metabolic activity of the specific fat depots in question may play a role. Because of the limited size and number of studies evaluating cryolipolysis in clinical populations, it is unclear which treatment sites are most amenable to cryolipolysis. Future comparative outcome studies should be adequately powered to determine which treatment sites are most suitable for fat reduction with this modality.
Because cryolipolysis is still a relatively new procedure, treatment protocols have yet to be optimized to maximize results. Recent studies have focused on maximizing the reduction of adipose tissue by adjusting treatment protocols. Three studies assessed the theoretical enhanced efficacy with multiple treatments in the same anatomic area and demonstrated that a second successive course of cryolipolysis treatment led to further fat reduction.13,23 It is important to note that although a subsequent treatment leads to further fat reduction, the extent of improvement was not as dramatic as the first treatment. Interestingly, one study demonstrated that a second treatment enhanced fat layer reduction in the abdomen area but not the love handles.13 One hypothesis for the diminished effect of the second treatment may be that the fat exposed to the second heat extraction is closer to the muscle layer. The vascular supply to the muscle layer may impede the efficiency of heat extraction so that the fat closer to the muscle layer may not reach the intended optimal temperature of 4°C. Another hypothesis is that adipocytes that survived the first treatment have a higher tolerance to cold.
Boey and Wasilenchuk evaluated whether the addition of a posttreatment manual massage enhanced the efficacy of a single cryolipolysis treatment.12 Immediately after treatment, patients received a 2-minute manual massage. This consisted of 1 minute of vigorous kneading of the treated tissue between the thumb and fingers followed by 1 minute of circular massage of the treated tissue against the patient’s body. To examine the effects of massage on subcutaneous tissue over time, histological analysis was completed through 4 months after treatment. Although the difference at 2 months after treatment was statistically significant, the difference at 4 months after treatment was not. One hypothesis for potentially improved efficacy with manual massage is that manual massage caused an additional mechanism of damage to the targeted adipose tissue immediately after treatment, perhaps from tissue-reperfusion injury. Histological analysis revealed no evidence of necrosis or fibrosis resulting from the massage, thus showing posttreatment manual massage to be a safe and effective method to further reduce the fat layer after cryolipolysis. Sasaki et al. described cryolipolysis with 5 minutes of posttreatment integrated preset mechanical massage using the device applicator with excellent outcomes.20
A low profile of adverse effects is one of the main advantages with cryolipolysis, especially when compared with more invasive measures. Only mild, short-term side effects, such as erythema, bruising, changes in sensation, and pain, were reported in the studies reviewed. Erythema was noted in multiple studies immediately after the treatment and subsided within a week.18–20 This is most likely because of the strength of the vacuum and the temperature at which the tissue is kept for extended durations and poses no threat to the patients. Swelling and bruising of the area were shown to a slightly lesser extent than erythema, but are believed to be because of the same processes. These complications also subsided shortly after.13,16,18,19 Hypersensitivity and hyposensitivity were shown in studies but were never debilitating nor persisted beyond 1 month. Coleman et al. demonstrated that patients exhibiting reduction in sensation recovered normal sensation in 3.6 weeks.21 This study also showed that a nerve biopsy taken at 3 months after treatment showed no long-term changes to nerve fibers, concluding that temperature and duration of cryolipolysis have no permanent effect on nervous tissue.21 In one study, pain during the procedure was generally nonexistent to tolerable 96 percent of the time.18
Rare side effects that have been described include vasovagal reaction18 and paradoxical adipose hyperplasia.24 Jalian et al. estimated an incidence of 0.0051 percent, or approximately one in 20,000, for paradoxical adipose hyperplasia.24 Affected patients exhibit fat loss after therapy and then develop a large, demarcated, tender fat mass at the site 2 to 3 months later. The hypothesized pathogenesis includes recruitment of stem cells and hypertrophy of existing fat cells in the area.24 However, compared with traditional liposuction side effects, cryolipolysis poses a minor threat to patients, with a very low incidence of complications.
Of note, the reviewed studies used a variety of different modalities to determine the degree of fat reduction after cryolipolysis treatments. Various studies have compared caliper, ultrasound, three-dimensional imaging, and manual tape measurements. Although no single study has compared all of these modalities, the available data suggest that these techniques correlate well with one another.30,31 Studies that used more than one of these modalities to assess outcomes after cryolipolysis also demonstrated that these measurements corresponded well.19,20
A drawback of this work is the limited number of high-quality, prospective, randomized clinical studies. Cryolipolysis was first described in 2007, and although its popularity has increased dramatically, the available literature remains limited. Tremendous variability exists in study design, machinery used, and outcome measures. Because of this lack of uniformity, comparing effect size becomes challenging, and the value of a meta-analysis of the available data is limited. The variations in the available studies make it difficult to control for any bias present in the discussed studies. Despite these limitations, clinical data demonstrate consistent fat reduction in treated subjects, which supports the clinical utility of this technique.
CONCLUSION
This study presents the first systematic review of the available data on cryolipolysis. Although the body of evidence is limited because of the nascence of this procedure, cryolipolysis is a promising procedure for nonsurgical fat reduction and body contouring. While the outcomes of cryolipolysis are rather modest, this technology is well suited for patients who desire nonsurgical spot reduction at modestly sized adiposities. Cryolipolysis appeals to both men and women and is an effective means by which new patients can be drawn to the aesthetic surgery practice.32 Although the specific mechanism of cryolipolysis has not been completely elucidated, this procedure appears to be effective and safe in the short term, with a limited side effect profile. Posttreatment manual massage has the potential to improve the efficacy of cryolipolysis. Multiple treatments in the same anatomic area may lead to further fat reduction, although the efficacy of cryolipolysis appears to be attenuated with successive treatments. The efficacy of this technique in areas that have been treated previously with liposuction remains to be studied. Future studies should address which treatment sites are most amenable to cryolipolysis to enhance treatment stratification for body contouring patients and should evaluate a potential role for cryolipolysis in skin tightening and the treatment of cellulite.
REFERENCES
- Berntorp E, Berntorp K, Brorson H, Frick K. Liposuction in Dercum’s disease: Impact on haemostatic factors associated with cardiovascular disease and insulin sensitivity. J Intern Med. 1998;243:197–201.
- González-Ortiz M, Robles-Cervantes JA, Cárdenas-Camarena L, Bustos-Saldaña R, Martínez-Abundis E. The effects of surgically removing subcutaneous fat on the metabolic profile and insulin sensitivity in obese women after large-volume liposuction treatment. Horm Metab Res. 2002;34:446–449.
- Rao RB, Ely SF, Hoffman RS. Deaths related to liposuction. N Engl J Med. 1999;340:1471–1475.
- Cardenas-Camarena L. Lipoaspiration and its complications: A safe operation. Plast Reconstr Surg. 2003;112:1435–1441; discussion 1442-1433.
Thomas M, Menon H, D’Silva J. Surgical complications of lipoplasty: Management and preventive strategies. J Plast Reconstr Aesthet Surg. 2010;63:1338–1343. - Fischer JP, Wes AM, Serletti JM, Kovach SJ. Complications in body contouring procedures: An analysis of 1797 patients from the 2005 to 2010 American College of Surgeons National Surgical Quality Improvement Program databases. Plast Reconstr Surg. 2013;132:1411–1420.
- Mulholland RS, Paul MD, Chalfoun C. Noninvasive body contouring with radiofrequency, ultrasound, cryolipolysis, and low-level laser therapy. Clin Plast Surg. 2011;38:503–520, vii.
- Duncan WC, Freeman RG, Heaton CL. Cold panniculitis. Arch Dermatol. 1966;94:722–724.
- Epstein EH, Jr, Oren ME. Popsicle panniculitis. N Engl J Med. 1970;282:966–967.
- Rotman H. Cold panniculitis in children: Adiponecrosis E frigore of Haxthausen. Arch Dermatol. 1966;94:720–721.
- Manstein D, Laubach H, Watanabe K, Farinelli W, Zurakowski D, Anderson RR. Selective cryolysis: A novel method of non-invasive fat removal. Lasers Surg Med. 2008;40:595–604.
- Boey GE, Wasilenchuk JL. Enhanced clinical outcome with manual massage following cryolipolysis treatment: A 4-month study of safety and efficacy. Lasers Surg Med. 2014;46:20–26.
- Shek SY, Chan NP, Chan HH. Non-invasive cryolipolysis for body contouring in Chinese: A first commercial experience. Lasers Surg Med. 2012;44:125–130.
- Bernstein EF. Longitudinal evaluation of cryolipolysis efficacy: Two case studies. J Cosmet Dermatol. 2013;12:149–152.
- Ferraro GA, De Francesco F, Cataldo C, Rossano F, Nicoletti G, D’Andrea F. Synergistic effects of cryolipolysis and shock waves for noninvasive body contouring. Aesthetic Plast Surg. 2012;36:666–679.
- Lee KR. Clinical efficacy of fat reduction on the thigh of Korean women through cryolipolysis. J Obes Weight Loss. 2013;3:1–5.
- Riopelle JT, Kovach B. Lipid and liver function effects of the cryolipolysis procedure in a study of male love handle reduction. Lasers Surg Med. 2009;82
- Dierickx CC, Mazer JM, Sand M, Koenig S, Arigon V. Safety, tolerance, and patient satisfaction with noninvasive cryolipolysis. Dermatol Surg. 2013;39:1209–1216.
- Garibyan L, Sipprell WH, III, Jalian HR, Sakamoto FH, Avram M, Anderson RR. Three-dimensional volumetric quantification of fat loss following cryolipolysis. Lasers Surg Med. 2014;46:75–80.
- Sasaki GH, Abelev N, Tevez-Ortiz A. Noninvasive selective cryolipolysis and reperfusion recovery for localized natural fat reduction and contouring. Aesthet Surg J. 2014;34:420–431.
- Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J. Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg. 2009;33:482–488.
- Kaminer MW, Newman J, Allison J. Visible cosmetic improvement with cryolipolysis: Photographic evidence. Paper presented at: 2009 Annual Meeting of the American Society for Dermatologic Surgery; October 1-4, 2009; Phoenix, Ariz.
- Pinto HR, Garcia-Cruz E, Melamed GE. A study to evaluate the action of lipocryolysis. Cryo Letters. 2012;33:177–181.
- Jalian HR, Avram MM, Garibyan L, Mihm MC, Anderson RR. Paradoxical adipose hyperplasia after cryolipolysis. JAMA Dermatol. 2014;150:317–319.
- Dobke MK, Hitchcock T, Misell L, Sasaki GH. Tissue restructuring by energy-based surgical tools. Clin Plast Surg. 2012;39:399–408.
- Jalian HR, Avram MM. Cryolipolysis: A historical perspective and current clinical practice. Semin Cutan Med Surg. 2013;32:31–34.
- Pinto H, Arredondo E, Ricart-Jane D. Evaluation of adipocytic changes after a simil-lipocryolysis stimulus. Cryo Letters. 2013;34:100–105.
- Preciado JA, Allison JW. The effect of cold exposure on adipocytes: Examining a novel method for the non-invasive removal of fat. Cryobiology. 2008;57:327.
- Avram MM, Harry RS. Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med. 2009;41:703–708.
- Cohen SR, Weiss ET, Brightman LA, et al. Quantitation of the results of abdominal liposuction. Aesthet Surg J. 2012;32:593–600.
- Selkow NM, Pietrosimone BG, Saliba SA. Subcutaneous thigh fat assessment: A comparison of skinfold calipers and ultrasound imaging. J Athl Train. 2011;46:50–54.
- Stevens WG, Pietrzak LK, Spring MA. Broad overview of a clinical and commercial experience with CoolSculpting. Aesthet Surg J. 2013;33:835–846.
- Brightman L, Geronemus R. Can second treatment enhance clinical results in cryolipolysis? Cosmetic Derm. 2011;24:85–88.
- Dover J, Burns J, Coleman S, et al. A prospective clinical study of noninvasive cryolypolysis for subcutaneous fat layer reduction—Interim report of available subject data. Presented at the Annual Meeting of the American Society for Laser Medicine and Surgery; April 2009; National Harbor, Md.
- Klein KB, Zelickson B, Riopelle JG, et al. Non-invasive cryolipolysis for subcutaneous fat reduction does not affect serum lipid levels or liver function tests. Lasers Surg Med. 2009;41:785–790.
- Rosales-Berber IA, Diliz-Perez E. Controlled cooling of subcutaneous fat for body reshaping. Presented at the 15th World Congress of the
- International Confederation for Plastic, Reconstructive and Aesthetic Surgery; 2009; New Delhi, India.
- Dover J, Kaminer M, Teahan M, Barrett L. Patient satisfaction at 2 and 6 months after a single non-invasive cryolipolysis treatment for subcutaneous fat layer reduction. Lasers Surg Med. 2011;43:968.
