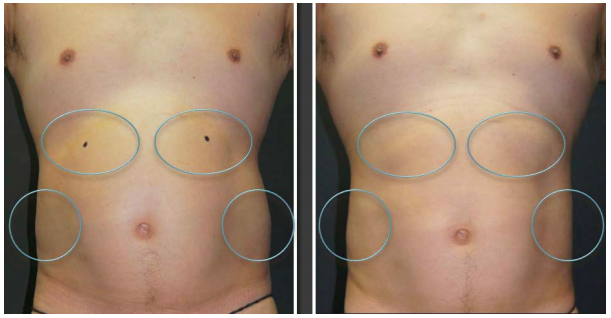
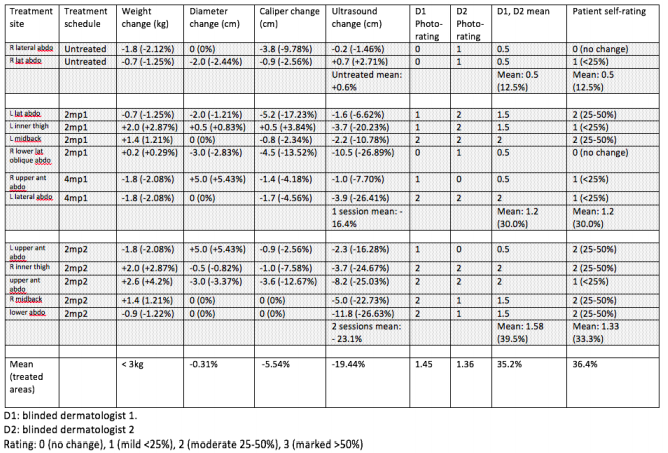
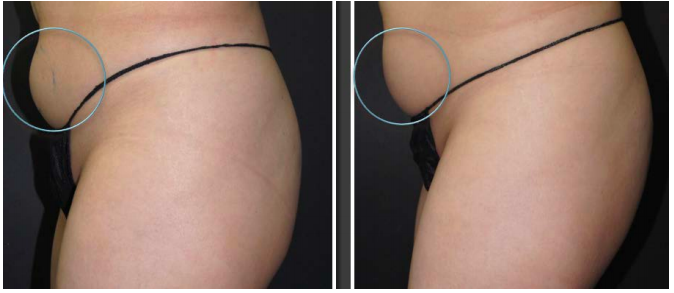
The subject demographics were: 6 females and 2 males, age range: 36 – 60 years old (mean: 46.8 years old). One subject was excluded from the study because of an unrelated traumatic injury to the shoulder requiring surgery. Of the 7 subjects, a total of 13 sites were treated: 3 subjects requested treatment at 2 body sites, 2 subjects had 1 site treated, and 1 subject had 4 sites treated. The lateral abdomen was the most commonly nominated site (figure 1). The specified measurements were done at baseline, 2-months and 4-months post-treatment (table 1). The most consistent record of body contouring change was photographic assessment and ultrasonic fat measurements, where the mean global ultrasonic fat reduction across all subjects was -19.44% (control: +0.62%) (table 1). Fat reduction across the 3 treatment groups (control, single treatment, double treatment) appear to correlate with the ultrasound measurements of +0.62%, -16.43% and -19.44% respectively. The calliper and circumference measurements correlated poorly with the clinical changes, with mean global reduction of -5.54% and -0.31% respectively for the enrolled subjects. Independent blinded physician (dermatologists) assessment of localised fat reduction was -30.0% after 1 treatment and -39.5% after 2 treatments, based on a mean 4-point rating scale (table 1). There was close concordance between the blinded dermatologists global score: 1.45 and 1.36 (mean 1.41), representing a mean global reduction of -35.2% on the 4-point rating scale (control: -12.5%).